Injuries have a significant impact on development beginning in infancy, reaching a peak during the adolescent and young adult years, but persisting in importance throughout the life span. Most experts no longer use the term “accidents,” when referring to these events. Based on its Latin roots, accident refers to an event that happens unexpectedly or by chance. As scientists and others have studied this problem over the past 50 years, it has become clear that many of these events do not occur by chance, but are predictable, based on the individual and environmental circumstances.
William Haddon, a physician/scientist, built upon the wealth of injury research stemming from World War II to describe a framework that has become central to understanding the causes and consequences of injuries. Haddon recognized that a phenomenon common to most injuries is the transfer of energy— thermal, radiant, chemical, electrical, and mechanical— in amounts that are too great or at rates that are too high for the body to absorb, hence an injury results. For example, when a motor vehicle collides with a tree or a streetlamp, the mechanical/kinetic energy of the vehicle is transferred to the driver or passengers, causing an injury such as a fractured arm or head trauma. The faster a car is going, the more energy it transfers in a collision. A safety belt or airbag absorbs much of that energy, decreasing the severity of injury. Another example would be a burn. When a child exploring a sink or tub turns on the hot water, the temperature setting may be so high that the transfer of that heat energy to the child’s hand or face results in a scald. Interestingly, the absence or lack of energy can also result in an injury. Many poisons, for example, act by disrupting the normal biochemical processes in the body.
In order to understand these transfers of energy with a view toward preventing injuries, Haddon created a two-dimensional matrix (Table 1). One dimension consists of the characteristics of individuals, their environments, and the particular type of energy or agent in question. Individual characteristics include age, developmental stage, physical or mental disabilities, and gender. One individual characteristic that has been the source of much debate is “injury proneness.” Although studies have examined aggressiveness, hyperactivity, and other behavioral characteristics with a view toward defining “proneness,” conclusions are inconsistent. Environments consist of the physical and social circumstances in which individuals find themselves. For example, an elderly woman, already at risk of hip fracture by virtue of her age, would have a much higher risk in an icy, wintry climate compared to a warmer climate. The energy or agent is specific to a particular injury. For example, roadways, sites of motor vehicle crashes, could have well-designed shoulders, improved lighting, proper grading and curves and many other environmental alterations to decrease injuries, even if the driver of a motor vehicle loses control for some reason. The second dimension reflects three stages in the timing of the transfer of energy—pre-event, event, and postevent. For example, the speed of a motor vehicle, combined with its size or mass, generates energy as it cruises along a road, prior to a crash (the pre-event phase). When a crash occurs, the energy is transferred to the driver and passengers (event phase). In the post-event phase, the effects of the transfer of energy can be lessened by appropriate emergency care and rehabilitation.
Understanding the interaction among the agent, host, and environments is key to injury prevention.
Table 1 Haddon Matrix to Consider Ways to Decrease the Risk of Motor Vehicle Injuries for Teenage Drivers
From a developmental perspective, strategies that minimize the need for individual actions are more effective in preventing injuries than strategies that expect individuals to act repeatedly. For example, passive restraints such as automatic safety belts and airbags are more effective than restraints that depend on individual behavior each time one enters a motor vehicle. Installing energy-absorbing materials on playgrounds is more effective than expecting parents to maintain constant vigilance as their children explore climbing equipment and develop new skills.
Within the overall problem of injuries, there are two major categories—unintentional and intentional. Intentional injuries refer to willful, deliberate actions that result in harm. Homicides represent intentional injuries in which one individual willfully attempts to kill or harm another individual. Suicides represent intentional injuries in which an individual attempts or succeeds in harming himself or herself. Unintentional injuries refer to those events that occur without a willful goal to do injury or harm. Most of what have commonly been referred to as “accidents” are unintentional injuries. The focus of this entry is unintentional injuries. Homicide and suicide are covered in other entries.
Overview Of Injuries Across The Life Span
There are many indicators to describe the outcomes of injuries. Because deaths are a basic component of public systems of vital statistics (i.e., deaths, births, marriages, divorces), deaths due to injuries are a commonly used indicator of the injury problem. Each year, there are approximately 100,000 deaths due to unintentional injuries in the United States— overall, a relatively small fraction of the more than 2.4 million deaths that occur. Looked at in alternative ways, however, injuries represent a significant health event for many ages. For example, about 27 million individuals visit an emergency department for an injury each year, representing just less than 10% of the entire population. Further, as shown in Table 2, after the first year of life, unintentional injuries are the leading cause of death through the young adult years. While injuries decline in rank after the age of 35, more than 36,000 adults between the ages of 35 and 64 die of injuries each year. It is only after the age of 45 that unintentional injuries begin to decline in importance as a cause of death compared to heart disease, cancer, and other chronic diseases.
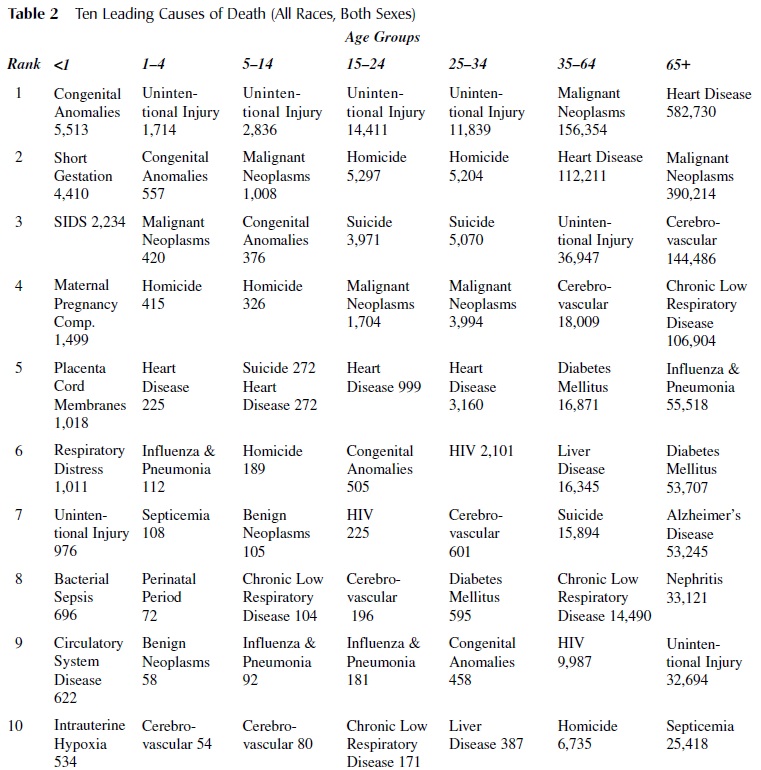 Table 2 Ten Leading Causes of Death (All Races, Both Sexes)
Table 2 Ten Leading Causes of Death (All Races, Both Sexes)
Other indicators of injuries include rates of hospitalization, visits to emergency departments, visits to physicians/clinics, and reports from individuals in community surveys about injuries that did not require contact with the health system. Table 3 shows that, of all injuries, falls are the leading cause of visits to hospital emergency departments across the age spectrum, except for adolescents and young adults. In general, deaths due to injuries represent just a small piece of the picture, with 40 to 50 hospitalizations and more than 1,000 emergency department visits for every death.
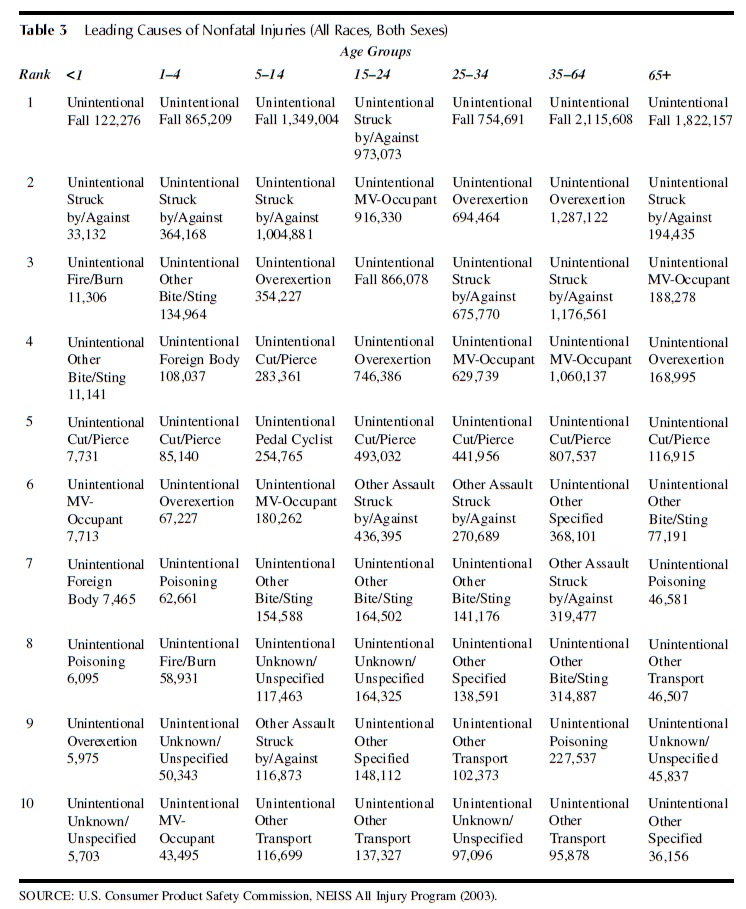 Table 3 Leading Causes of Nonfatal Injuries (All Races, Both Sexes)
Table 3 Leading Causes of Nonfatal Injuries (All Races, Both Sexes)
Although Tables 2 and 3 provide an overall picture of injuries, it is important to point out that males are at greater risk of injury for virtually every type of injury, throughout the course of life. Physical, psychological, and cultural factors all may play a role in this increased risk for males.
Alcohol
Any review of the issue of injuries must consider the role of alcohol. Alcohol has profound and subtle effects on the physical, cognitive, and social characteristics of individuals, so it is not surprising that use of alcohol is one of the most important injury risk factors. In 2000, the per capita consumption of alcohol was estimated at nearly 290 cans of beer, 60 glasses of wine, and 133 shots of spirits. Although consumption of alcohol is widespread, it is calculated that about 10% of the population is responsible for 50% of alcohol use. Decreasing the use of alcohol would be one of the most effective strategies to decrease the toll that injuries take on health. Alcohol is associated with over 30% of fatal motor vehicle crashes, accounting for nearly 13,000 of the 42,000 traffic-related fatalities in 2000. Adults between the ages of 25 and 44 are at greatest risk for alcohol-related motor vehicle deaths, with 44% of traffic fatalities involving alcohol. For 16to 24-year-olds, alcohol is involved in 30% of fatalities in contrast to only 4.7% for those older than age 65. It is noteworthy that many motor vehicle deaths for teens involve alcohol, even though every state prohibits alcohol consumption younger than age 21. Even for children, alcohol represents a substantial risk for motor vehicle–related deaths. Annually, of the approximately 2,800 children under the age of 16 who die in motor vehicle–related events, 20% involve drinking drivers. About 60% of the deaths involve children as passengers in cars and the other 40% involve them as pedestrians or bicyclists. For the children who die as passengers in alcohol-related crashes, more than two thirds are in cars in which their own driver had been drinking alcohol. Alcohol has also been associated with other injuries. For example, burns and smoke-related injuries and deaths from fires, especially in homes, often involve alcohol. Similarly, the risk of falls, the leading cause of hospitalization for injuries, is understandably increased by alcohol consumption. Alcohol is associated with a significant proportion of drownings. Given the important role that alcohol consumption plays in injury-related deaths and disabilities, policy efforts to control alcohol are key to reducing injuries.
Infants And Toddlers
The interaction among host and environmental characteristics of infants is unique and complicated. Infants begin their lives entirely dependent on the behaviors and actions of their parents or other caretakers with regard to the relationship to their environments. As they develop during the first year, however, two changes take place. First, as their brains and neuromuscular systems develop, infants are able to exert more control over their behavior. Second, parents must learn to become more attentive to these newly emerging capabilities. The interaction between these two phenomena explains why unintentional falls are the leading cause of nonfatal injuries for this age group. Falls from changing tables, for example, may result from the newly emerging and perhaps first expression of the ability to roll over combined with a momentary distraction by a parent as they reach for a diaper. Agran and colleagues actually looked more precisely at the relationship between development and injury hospitalization by examining rates in 3-month intervals, rather than the usual 1-year or several-year age categories. They found, for example, that indeed the risk for injury rises markedly between 9 and 11 months. Rapid and complex developmental processes are associated with a variety of injuries beyond the first year of age. Agran reported that for children under 4, injury rates peaked at 15 to 17 months. The types of falls varied greatly, again reflecting the different exposures that are associated with increasing physical and developmental capacities. Falls from stairs were prominent for the youngest children, giving way to falls from playground equipment as they moved into this new environment. Poisoning due to medications was the greatest risk at 21 to 23 months before declining in importance.
Even for infants and toddlers the overall risk of injury differs markedly between boys and girls.
Young Children
The beginning of school represents a developmental milestone that is accompanied by its share of injury risks. Motor vehicle injuries are the leading injury, but especially between the ages of 5 and 14, pedestrian injuries represent a significant risk. Recent data show that the pedestrian death rate for 5to 9-year-olds was 1.36 compared to 1.85 for motor vehicle occupants. For 10to 14-year-olds the rates were 1.23 and 2.80, respectively. Children of this age are only beginning to develop the ability to judge the distance and speed of a moving vehicle. In addition, these children are likely to dart into the traffic, even if they happen to be at an appropriate safety crossing.
Several prevention strategies have had remarkable impacts on injury deaths and disabilities for children. Each of these strategies is designed around an understanding of the physical and developmental characteristics of this age group. For example, the design of child safety seats recognizes the need to restrain children in ways that are both secure, comfortable, and, for parents, convenient. When used correctly, safety seats reduce the risk of death and serious injury by 70%. Since the implementation of the first child safety seat law in Tennessee in 1978, hundreds of children have been spared death or serious injury in motor vehicle crashes. Recently, many states have passed laws requiring booster seats for children up to 80 pounds out of recognition that adult safety belts do not adequately correspond to the anatomic characteristics of children. The Poison Prevention Packing Act of 1970 regulates access to containers and other features of hazardous substances, building upon an understanding of the exploring behaviors of toddlers and young children coupled with the difficulty that parents and other caretakers have in vigilantly monitoring these youngsters. Fencing for swimming pools, requirements that children wear bike helmets, regulation of hot water heater temperatures, and other interventions are most effective when they take into account the developmental stages of those children most at risk.
Adolescents
The collision of the developmental tasks of adolescents with their physical and social environments makes it possible to understand the high rates of injury death and disability in this age group. Establishing autonomy, becoming comfortable with pubertal changes, building relationships outside the family, and developing abstract reasoning abilities all combine to increase the risk of injuries. In contrast to school age and early adolescence, where the injury-related death rate is about 8.9 per 100,000 population, the rate markedly increases to nearly 40 per 100,000 for 15to 24-year-olds, and then begins to decline.
Driving is perhaps the most important symbol of adolescence. The use of a motor vehicle gives expression to growing feelings of independence and facilitates interactions with new friends and groups. Motor vehicles, with their capacity to generate and thus transfer huge amounts of energy, create a challenge in view of the rapid and sometimes intense physiological and psychological developments for adolescents.
The National Youth Risk Behavior Survey (YRBS) is a school-based, nationally representative survey of over 15,200 students in grades 9 through 12. The YRBS identifies many behaviors that reflect how adolescent development increases the risks of injury. Nationally, over 18% of students had rarely or never worn seat belts when riding in a car. During the 30 days preceding the survey, 30% of students had ridden with a driver who had consumed alcohol and 12% had themselves driven after drinking alcohol.
Given the complex interaction between the driver, the motor vehicle, and the external environment, adolescents, and particularly new drivers, are especially at risk. Safe driving requires a level of maturity that is heavily dependent on time as well as experience with the multiple and frequently changing circumstances that drivers encounter. Motor vehicle crashes account for nearly 40% of all deaths for 15to 19-year-olds, over 2,600 deaths per year. Sixteen-year-old drivers are involved in 42 crashes per million miles driven compared to 30 and 15 for 17and 18-year-olds, respectively. Approximately 25% of 16-year-olds are involved in a crash in any given year.
In order to address the risk of death and injury for new drivers, over 40 states have adopted graduated driver license (GDL) programs, interventions that reflect the developmental needs of adolescents. Basically, GDL places restrictions on new young drivers and gradually removes those restrictions as they gain maturity and experience. For example, in North Carolina, individuals obtain a Level 1 permit at the age of 15 that allows them to drive as long as there is an adult supervisor in the front seat with them. For the first 6 months, the new driver is restricted to the hours of 5 a.m. to 9 p.m., to gain important experience during the more forgiving driving conditions of daylight, before being exposed to driving during the nighttime hours. After 1 year of supervised driving, new young drivers are permitted to drive by themselves, but only until 9 p.m. for 6 months. In addition, during this 6-month period of newly unsupervised driving, only one passenger is permitted, because for 16-year-olds, two passengers more than double the risk of a crash, and three passengers increase the risk by nearly fivefold. GDL programs, incorporating an understanding of adolescent development, have had remarkable effects, such as a 25% reduction in deaths for 16-year-old drivers.
Adults
During adulthood, the death rate due to unintentional injuries remains relatively stable at around 30 to 32 per 100,000 population, with motor vehicle injuries accounting for at least half of these deaths. After the age of 35 years, injuries fall to second behind cancer as a cause of death.
The workplace is obviously an important environment to consider in describing injuries during the productive adult years. For younger adults (20–34 years), workplace fatalities average 1,760 per year (3.9 per 100,000 population), while for adults 35 through 54, the rate increases to 4.5. Approximately 18% to 19% of these deaths are associated with assaults (intentional injuries). Reflecting the contribution of motor vehicle injuries to overall mortality, transportation incidents account for 40% of occupational deaths. Untoward encounters with equipment or other objects is responsible for the next most frequent cause of occupational death at 16%, with falls and exposures to harmful substances accounting for 9 to 12% of fatalities. Not surprisingly, the risks vary greatly by industry. Agriculture, forestry, and fishing have reported about 800 deaths per year in recent years for a rate of about 23.8 per 100,000, followed by mining with 150 deaths per year with a rate that has varied between 21.7 and 27.0 over the past several years. At the other end of the spectrum, finance, insurance, and real estate has experienced around 100 deaths per year at a rate of 1.2 per 100,000 population.
Age 65 And Beyond
The interaction between host and environmental characteristics results in particular risks for injuries among this age group. Physical characteristics include changes in vision, losses in strength, coordination and response times, and changes in bone density with increasing fragility. In addition to these developmental changes, many medications for hypertension, heart disease, and other chronic diseases may impede normal strength and reflexes. Complementing these changes in the elderly individual as the host are environmental characteristics. The problem is not changes in environments per se, but rather the failure to attend to safety hazards in the home or other locations. Climbing into a tub poses a minimal risk for a 40-year-old, but may create a sizable hazard for a 70-year-old. At night, the same darkened hallway that for years was second nature becomes a hazard as physical skills diminish. The ability to negotiate the complicated environmental interactions of driving is dependent on physical and cognitive skills that are in decline.
Injuries constitute only a fraction of deaths for seniors. For those between the ages of 65 and 74, the death rate is only 47 per 100,000 compared to 860 and 776 for cancer and heart disease, respectively. Beyond the age of 75, the differences in rates are even more dramatic. The mortality rate for injuries does increase to 146 per 100,000 population, but the rates for heart disease (3,100 per 100,000) and cancer (1,462 per 100,000) overshadow that rate.
In spite of the relative decline in importance of injuries in the later years, recognition of the physical and cognitive needs of elderly individuals can decrease the risks of disability and death. Regular health visits allow assessment of the capacities of elderly patients. Such visits should evaluate vision, balance, strength, and use of pharmaceuticals for other chronic diseases. Weight-training and other exercises, for example, may improve strength and gait. Screening for osteoporosis may identify those in need of attention to weakening bones, a risk factor for falls and fractures. Health care providers or indeed anyone who interacts regularly with the elderly should inquire about their physical environments as well, as a way to address injuries. Improvements in lighting, attention to potential obstacles, creation of nonslip surfaces, handles in tubs and showers, and many other interventions may decrease the risk of injury for individuals with physical impairments. Transportation, in particular, is a challenge. Safe driver programs for the elderly are an important approach. Development of alternatives for elderly individuals who drive themselves is a growing need as the overall population ages.
Summary
Injuries are a prominent health and behavioral outcome throughout the life span, becoming the leading cause of death after the first year and remaining the leading cause until well into adulthood. Even when injuries decline in rank, they are the source of death and disability for a large segment of the population. Perhaps the most significant aspect of injuries is that most of them are preventable with attention to the characteristics of individuals and their interactions with their physical and social environments. Deaths due to motor vehicle injuries, the leading cause, have declined by 38% during the past 50 years. This decline has resulted from interventions that are based on an understanding of the mechanisms of injuries as informed by the Haddon matrix combined with the political will and resources to effect environmental changes. In addition, interventions have enabled individuals to become more aware of the important role that they play in their interaction with environments. Across all causes of injuries, amelioration of individual and environmental risk factors has been associated with thousands of averted deaths and hundreds of thousands of cases of averted disability and distress. Given the ability to understand the factors associated with injuries, further substantial progress in reducing this cause of distress is desirable and feasible.
References:
- Agran, P., Anderson, , Winn, D., Trent, R., & WaltonHaynes, T. (2003). Rates of pediatric injuries by 3-month intervals for children 0 to 3 years of age. Pediatrics, 111,683–692.
- Foss, D., Feaganes, J., & Rodgman, E. (2001). Initial effects of graduated driver licensing on 16-year-old driver crashes in North Carolina. JAMA, 286, 1588–1592.
- Hall, , Fingerhut, L., & Heinen, M. (2004, November).National trend data on hospitalization of the elderly for injuries, 1979–2001. Presented at the annual meeting of the American Public Health Association, Washington, DC.
- National Center for Health Statistics. (2004). National trends in injury hospitalization, 1979–2001. Washington, DC: Centers for Disease
- National Vital Statistics System, http://www.cdc.gov/nchs/ nhtm Runyan, C. (2003). Introduction: back to the future—revisiting Haddon’s conceptualization of injury epidemiology andprevention. Epidemiology Review, 25, 60–64.
- Substance Abuse and Mental Health Services Administration. (2003). Percent reporting alcohol use in the past year by age group and demographic characteristics: NSDUH (NHSDA), 1994–2002.
- SAMHSA/OAS, Results from the 2002 National Survey on Drug Use and Health: National findings. DHHS Pub. No. (SMA) 03-3836. Retrieved from http://www.niaaa.nih.gov/databases/dkpat3.htm
- S. Consumer Product Safety Commission, NEISS All Injury Program, http://www.cpsc.gov/LIBRARY/neiss.html
- S. Department of Labor. (2002). Fatal occupational injuries in the United States, 1995–1999: A chartbook. Washington, DC: U.S. Bureau of Labor Statistics.
- Yi, , Williams, G. D., & Dufour, M. C. (2003). Surveillance report #65: Trends in alcohol-related fatal traffic crashes, United States, 1977–2001. Bethesda, MD: National Institute on Alcohol Abuse and Alcoholism, Division of Biometry and Epidemiology. Retrieved from http://www.niaaa.nih.gov/databases/crash01.htm