 Measuring and recording heart rate data is essential to the HZE program. In fact, without accurate data, developing a training plan is not possible. Students may use a number of different assessments to develop their training plans, each of which is valuable in and of itself. When combined and compared with others, these assessments can show trends and starting points, which students can then use to make healthy exercise decisions. This is the power of a heart monitor: it helps students make health and fitness decisions.
Measuring and recording heart rate data is essential to the HZE program. In fact, without accurate data, developing a training plan is not possible. Students may use a number of different assessments to develop their training plans, each of which is valuable in and of itself. When combined and compared with others, these assessments can show trends and starting points, which students can then use to make healthy exercise decisions. This is the power of a heart monitor: it helps students make health and fitness decisions.
Resting Heart Rate
Heart rate changes with the time of day, increasing during the daylight hours and decreasing during the night hours. Resting heart rate is the heart rate first thing in the morning, before getting out of bed. Because it measures parasympathetic nervous response, resting heart rate is one of the key indicators of overtraining or other stress.
Resting heart rate, sometimes referred to as a.m. heart rate, decreases as a result of positive training activities, meaning that as you get fitter, your heart works less to do the same work. A lower resting heart rate means less physiological stress on the heart muscle because it contracts fewer times. Although heart rate escalates dramatically during a training session, fitness training results in a lower resting heart rate, which translates to fewer contractions over the course of a lifetime. In other words, the heart of someone who exercises has to work less over that person’s lifetime. This is one of the training effect responses. The result of this training effect is that a person can save more than 700 million heartbeats over the course of a lifetime (learn more about this in appendix B). That’s quite a payoff in the long run.
Ambient Heart Rate
Ambient heart rate is frequently confused with resting heart rate. Ambient heart rate is measured when the person is awake but sedentary—for example, when resting in a sitting position while awake and involved in a sedentary activity such as working on a computer, watching television, or talking. Resting heart rate, on the other hand, is taken in bed before rising when the heart is at complete rest. Ambient heart rates change as a result of stimuli that influence heart rate including body position; external influences such as temperature, hydration, and food ingested; internal influences such as level of fatigue, stress, hunger, and sleep; and medication.
Ambient, or sitting, heart rate, like most heart measurements, is relative, not absolute. It is a number that needs to be compared to other ambient heart rate measurements. Taking ambient heart rates repeatedly gives a more accurate assessment than measuring it once. The normal range for ambient heart rate is usually between 50 and 90 bpm, but healthy ranges of ambient heart rates are very broad. The training effect is also seen in ambient heart rates. In other words, the fitter you become, the lower your ambient heart rate will be. Ambient heart rates under 60 bpm are rare. An ambient heart rate over 80 bpm may indicate a combination of various types of stress.
Delta Heart Rate
The famous poet David Whyte once wrote, “All things change when we do.” That’s the principle behind the delta heart rate assessment. Delta (Δ), a letter in the Greek alphabet, means “change.” Hence the delta heart rate, or orthostatic heart rate, is a measure of the heart’s response to a change in body position.
Heart rate alters with changes in body position. Its increase and decrease depends on the workload demand on the heart muscle. If you lie down, for example, your heart doesn’t have to work as hard as it does when you are standing because it doesn’t have to pump blood upward against the force of gravity. Likewise, a sitting position elicits a lower heart rate measurement than the standing position.
Stress can also affect heart rate. Thus, delta heart rate can be used as an indicator of current stress. If you are overtraining, are on the verge of a respiratory infection, are suffering from a lack of sleep, or have recently changed your diet, for example, your delta heart rate will be higher than normal. Competitive athletes commonly use delta heart rate as an indicator of overtraining or pending immune compromise.
The most common way to measure delta heart rate is to record the heart rate when lying down and then when standing. The difference (standing heart rate minus sitting heart rate) is the delta heart rate. The change in heart rate values results when the heart responds to different workloads. Because a healthy heart can adjust efficiently to small changes in work load, a higher delta heart rate might indicate a less fit cardio vascular system. However, it could also indicate stress from internal or external conditions. Once a person has recorded multiple readings, the delta heart rate measure can be used as an indicator of cardiovascular fitness or stress. In a lying position, the heart rate lowers to a value close to resting heart rate (figure 2.2, P).
When we stand up, the cardiac system adjusts to this change in body position: the heart rate increases and then drops. Eventually, usually after about two minutes, the heart rate hovers around a new value (figure 2.2, S). The change in heart rate, known as delta heart rate, is the difference between P and S. In figure 2.2, for example, the delta heart rate is 15 bpm (85 – 70 = 15).
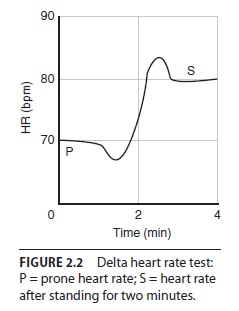
Figure 2.2 Delta heart rate test
Recovery Heart Rate
Recovery heart rate measures the heart’s ability to return to its normal rate after exercise. It is a trainable heart rate, meaning that the more fit one becomes, the more quickly the heart rate returns to preexercise rates once exercise is stopped. Recovery heart rate is the time between the cessation of exercise and the heart rate’s return to its preexercise level. A common recovery heart rate measurement is one to two minutes, although total recovery may require as long as an hour. The shorter the heart rate recovery is, the fitter the person is. There are two types of recovery heart rate measurements: intrarecovery heart rate (within a workout) and interrecovery heart rate (between workouts):
- Intrarecovery heart rate is the time it takes for the heart to recover within one workout session.
- Interrecovery heart rate is the time it takes for the heart and specific muscle groups to completely recover between workout sessions.
Ideally, students’ intrarecovery heart rates recover (i.e., return toward ambient heart rate) very quickly. Some call the interrecovery heart rate the one that falls like a stone; that’s how quickly it usually recovers. Interrecovery heart rates that are slow to recover can indicate a less-fit cardiovascular system or be a warning of heart-related conditions.
With conditioning and the use of mindful recovery, students can learn to improve their recovery heart rates. In fact, to some extent, they can learn to consciously regulate their heart rates. Mindful recovery is also an excellent tool for managing stressful situations.
Mindful recovery involves the use of visualization, deep breathing, body positioning, and similar relaxation techniques to purposefully lower the heart rate as rapidly as possible. With practice, students can develop their own relaxation strategies. There are two methods of mindful recovery:
- Active recovery, which involves continuing to move gently
- Passive recovery, which involves stopping all exercise
Maximal Heart Rate
Maximal heart rate (MHR) is the maximal number of times a heart can beat in one minute. The heart will only contract so fast—and not one beat faster—that’s why it’s called MHR. MHR is a fixed value, but everyone’s MHR is unique. Two 17-year-olds could have a difference in MHR as great as 40 bpm.
Measuring MHR is essential to HZE. It is the base, or anchor point, for setting zones and the core piece of information necessary for students to complete the HZE course.
Physical educators often teach their students the age-adjusted MHR formula, 220 – age (also known as the regression formula). This equation was developed in the early 1970s by scientists Fox, Naughton, and Haskell, who intended it to be only a rough formulation and not representative of an entire population. In 1992, Dr. Sam Fox, director of preventive cardiology programs at Georgetown University Medical Center, made this statement in a Chicago-Sun Times article: “The crude formulas that I am partly responsible for . . . are only crude first cuts” (February 2, 1992, p. 29). He developed the calculations with an associate, William L. Haskell, then a professor of medicine at Stanford University School of Medicine. Although the formula has become widely accepted, there are no clinical trials to support it and no published record of research to support it. Furthermore, in the sample, all subjects were male and under 55 years of age. Research has shown that people of the same age have widely varying MHRs, as much as 11 beats per minute, and that MHR in fit people changes very little as they age.
What We Know About Maximal Heart Rate
Maximal heart rate is a specific value: the maximal number of times the heart can contract in one minute. As a teacher, you need to know and explain to your students the following facts about MHR:
- It is genetically determined—that is, you are born with it.
- It is a fixed (absolute) number that does not decline with age unless you become unfit.
- It cannot be increased by training.
- It is not an indicator of current fitness.
- In young children, it is often measured at over 200 bpm.
- It tends to be higher in women than in men.
- It is affected by drugs.
- It is not fully developed until after puberty.
- It is not a predictor of athletic performance.
- It varies greatly among people of the same age.
- For most people, it cannot be accurately predicted by any mathematical formula.
- It does not vary from day to day, but it is test-day sensitive based on physical impacts that day, such as drugs or illness.
- Testing should be conducted multiple times to determine the correct number.
- It is sport specific.
- It is the basis for setting personal heart zones.
Measuring Maximal Heart Rate
Maximal heart rate is the best index to use in setting individual heart zones. Because it serves as the principal marker for exercise intensity, your students will anchor their heart zones around MHR.
There are a number of approaches to measuring this value. Fit people, under the supervision of a qualified instructor, sometimes undergo a maximal heart rate test, which involves exercising to the point of fatigue in two to four minutes to determine their true MHR number. Exercise intensity is increased regularly until the person cannot continue. In this program, however, students will take a series of submaximal heart rate tests and undergo an assessment below maximal effort, and then use the results to predict MHR.
MHR is sport specific. It is affected by factors such as the type and amount of muscle used, body position, and environment (e.g., water versus land). Following are some of the factors involved in determining the specific maximal heart rate for various sports:
- Body position
- Size and number of muscle groups involved in the activity
- Ambient temperature of the environment
- Type of activity, such as weight-bearing sports (e.g., running)
- Use of equipment (e.g., wheels in cycling).
Some of the lowest MHRs are recorded for swimming (a sport in the prone position), activities done in colder ambient temperatures, and activities that use the smaller upperbody muscle groups. The highest MHRs are recorded for weight-bearing activities (e.g., cross-country skiing), activities that use the large muscles of the body, and activities that use both the upper and lower-body muscle groups. People who work out in multiple sports need to determine their MHR for each because it varies by sport. However, the HZE program uses a global, all-sport MHR to set zones, which is easier for teachers and students to follow. A global MHR is accurate enough to use for all sport disciplines in the school environment.
Testing for Maximal Heart Rate
The submaximal heart rate assessments used during the HZE program are the 1-mile (1.6 km) walking test, talk test, biggest number test, step test, and chair test. The mathematical MHR formula has limitations and is less reliable than submaximal assessments.
Most methods used to determine MHR are valued or rated according to the ultimate use of the number obtained. Competitive athletes, for example, need very accurate numbers. The intention of the HZE program is to teach students the process for determining MHR. The numbers they get will be only estimates, and depending on the method used, the estimated MHR will vary. In the school setting, we are looking for a general all-sport maximum: a global fitness estimate, not a specific MHR for each sport activity.
MHR can be determined by exercising to a maximal intensity or by completing submaximal heart rate tests to estimate it. The most accurate method is a maximal test to near exhaustion, but this may not be practical in school settings and is difficult to do, particularly for the unfit. Thus, exercise scientists have developed a series of submaximal heart rate tests that can be used to predict MHR. These tests most often use a formula that predicts MHR based on age. The theory behind this formula for predicting MHR is that the maximal number of times our hearts can beat decreases as we age.
The original studies on MHR were conducted in the 1930s on fit young men and not fit older men. The results of those original studies are now being challenged. Several long-term studies of fit people indicate that MHR is related not to age, as many have believed for so long, but to lifestyle. For example, an active 30-year-old may have an MHR of 210 bpm. If, as that person ages, she simultaneously decreases physical activity and becomes sedentary, her MHR will likely decrease. If, however, she were to exercise at a moderate intensity regularly as she aged, her MHR would likely remain unchanged. Indeed, Dr. Dave Costill (1996) conducted studies that follow the same fit people over a period of 22 years. His findings show that MHR remained unchanged when his subjects exercised regularly at moderate intensity.
People who want to get fit may find that exercising at certain percentages of true or predicted MHR provides a variety of benefits, such as the following:
- Enhanced fat burning: Burning more fat and more total calories by training in different heart zones.
- Improved stamina: Going farther, faster, and longer because endurance fitness improves (called improved endurance capacity).
- Increased efficiency: Going farther on each calorie burned.
- Cardiovascular improvement: Transporting nutrients and oxygen throughout the body more efficiently.
- Psychological power: Increased alertness, mental stamina, and self-esteem.
At lower exercise intensities (i.e., lower heart zones), these benefits result in lowered blood pressure, reduced stress, and stabilized body weight. As the intensity of a workout increases (i.e., higher heart zones), the benefits of exercising change.
Post Views: 161